Are nasal steroids effective in children with adenoid
hypertrophy?
Fevzi Solmaz
1
, Mustafa Erhan Aşcıoğlu
2
, Osman Durgut
1
, Oğuzhan Dikici
1
, Mehmet
Haksever
1
, Davut Akduman
3
1
Department of Otorhinolaryngology, University of Health Sciences, Bursa Yüksek İhtisas Training and Research Hospital, Bursa,
Turkey
2
Department of Pediatry, University of Health Sciences, Bursa Yüksek İhtisas Training and Research Hospital, Bursa, Turkey
3
Department of Otorhinolaryngology, Düzce University School of Medicine, Düzce, Turkey
ABSTRACT
Objectives: Chronic nasal obstruction is a common disease of childhood. Adenotonsillar hypertrophy plays
an important role in obstructive sleep apnea. The topical use of the aerosolized forms of corticosteroids therefore
seems the most appropriate route to decrease systemic side effects. The aim of our study is to demonstrate the
effect of topical mometasone furoate especially on the adenoid volume in patients without any allergic story.
Methods:The study group consisting of 30 males and 25 females was administered topical nasal mometasone
furoate steroid treatment. The 20 patients were in the control group where saline solution (0.9% NaCl) treatment
was administered consisted of 12 males and 8 females. Nasopharyngeal X-rays before treatment revealed that
25 patients were Grade 2 and 30 patients were Grade 3 according to the Fujioka method.
Results:Flexible endoscopy performed before the treatment revealed that 20 patients were Grade 2, 11 patients
were Grade 3 and 24 patients were Grade 4. Nasal endoscopies performed after 6 weeks of intranasal topical
steroid therapy revealed that 45 patients were Grade 1 and 10 patients were Grade 2. A statistically significant
difference was present between endoscopic grades before and after treatment (p < 0.0001). Nasal endoscopies
performed after 6 weeks in control group receiving saline solution treatment revealed Grade 2 in 7 patients,
Grade 3 in 10 patients and Grade 4 in 3 patients. There was no statistically significant difference between in
the prior and later grades of the control group (p = 0.3125).
Conclusions:We believe that the use of intranasal steroids (mometasone furoate) for 6 weeks in patients with
pediatric chronic nasal obstruction due to adenoid hypertrophy may be an effective treatment modality in
alleviating symptoms and decreasing adenoid volume without causing systemic side effects.
Keywords:Nasal steroids, adenoid hypertrophy, flexible endoscopy, nasopharyngeal X-rays, Fujioka method
Address for correspondence: Fevzi Solmaz, MD., University of Health Sciences, Bursa Yüksek İhtisas Training and Research Hospital, Department of
Otorhinolaryngology, Bursa,Turkey
E-mail: [email protected], Tel: +90 224 295 50 00, Fax: +90 224 366 04 16
Copyright © 2019 by The Association of Health Research & Strategy
Available at http://dergipark.gov.tr/eurj
The European Research Journal 2019;5(2):311-318
hronic nasal obstruction (CNO) is a common dis-
ease of childhood with an estimated prevalence
of 2-3% in the healthy pediatric population [1]. Ade-
notonsillar hypertrophy plays an important role in ob-
structive sleep apnea (OSA) pathophysiology and
reaches its peak incidence between the ages of 2 and
8 years [2, 3]. OSA is the result of increased airway
resistance during sleep and characteristically manifests
as repeated arousals, hypercapnia, episodic snoring,
and periods of oxyhemoglobin desaturation [4]. Ade-
C
ORIGINAL ARTICLE
e-ISSN: 2149-3189
DOI: 10.18621/eurj.405439
Received: March 13, 2018; Accepted: October 13, 2018; Published Online: November 8, 2018
The European Research Journal
Volume 5
Issue 2
March 2019 311

Eur Res J 2019;5(2):311-318 Topical nasal steroid and adenoid hypertrophy
notonsillar hypertrophy is the most common cause of
OSA in preschool children [5]. Allergic exacerbations
give rise to the hypertrophy of adenoid tissue but re-
peated upper respiratory tract infections(URTIs) may
also be the cause.
The hypertrophied lymphoid tissue may cause
many pathological conditions including snoring, sleep
apnea, sinusitis otitis media with effusion and adenoid
face [6]. If left untreated, OSA may cause many seri-
ous problems such as cognitive and behavioral disor-
ders, systemic and pulmonary hypertension, enuresis,
and developmental delay [7]. Adenoidectomy is the
definitive treatment modality for upper airway ob-
struction caused by adenoid hypertrophy but decon-
gestant nasal drops have also been used for its
symptomatic management [8].
Structural and neuromuscular pathologies may
also cause CNO but the main factor in the pathogene-
sis of pediatric CNO is the size of the tonsils and ade-
noid tissue making their surgical excision the primary
choice of treatment [9, 10]. Postoperative residual
OSAS is found in 20% of the children who have un-
dergone adenotonsillectomy [11].
The nonsurgical treatment options for pediatric
CNO are attracting increasing attention due to the po-
tential complications of adenotonsillectomy. Anti-al-
lergic drugs have been used from time to time despite
the lack of adequate evidence to support their usage,
as allergy is just one of the reasons for obstruction
[12]. The efficacy of oral steroids in relieving the ob-
structive symptoms of adenoid hypertrophy is reported
in the literature. They also reduce the size of the ade-
noid tissue significantly. However, their long-term use
is limited due to the significant side effects [12]. The
topical use of the aerosolized forms of corticosteroids
therefore seems the most appropriate route to decrease
systemic side effects, since there will be a minimal
amount of systemic absorption from the upper airway
[13]. The 6-week administration of triamcinolone ace-
tonide aqueous nasal spray to children with allergic
rhinitis aged 6 to 12 years has been reported to have
no significant impact on adrenocortical function.
Treatment with mometasone furoate aqueous nasal
spray (200 micrograms once a day) for 14 days was
shown to be safe and well-tolerated in children [14].
Local and systemic inflammatory markers and
proinflammatory cytokines, which trigger lymphoid
tissue proliferation, are increased in children with ade-
notonsillar hypertrophy. Systemic or topical anti-in-
flammatory agents have therefore been recommended
to prevent the potential tonsillar hypertrophy in these
patients [15, 16]. Topical nasal corticosteroids can al-
leviate CNO symptoms and nasal obstruction as well
as reduce the size of the adenoid tissue [17, 18]. How-
ever, the optimal dose and duration of treatment with
nasal steroid agents is not clearly defined yet.
The current inadequate evidence on the efficacy of
intranasal steroids in children with adenoid hypertro-
phy and nasal obstruction led us to conduct this study.
With this study we evaluated the efficacy of Mometa-
zon furoat (topical nasal steroid) on adenoid hypertro-
phy in children.
METHODS
Patients
The study was conducted a randomized placebo-
controlled children with adenoid hypertrophy who
presented to Otolaryngology and Pediatrics outpatient
clinics of our hospital. All procedures performed in
studies involving human participants were in
accordance with the ethical standards of the
institutional and/or national research committee and
with the 1964 Helsinki declaration and its later
amendments or comparable ethical standards. The
Institutional review board (IRB) was taken for the
patients (Number: 66519339- 900-01/1304). Informed
consent was obtained from all individual participants
included in the study. Adenoidectomy operation under
general anesthesia was suggested as the main
treatment of adenoid hypertrophy to all parents or
patients and they were informed about the possible
complications of the operation. Mometazon furoat as
topical nasal steroid was prescribed for the patients
who rejected the surgery and for the relief of
symptoms in case of preoperative severe symptoms.
All the patients included in the study had a complaint
of snoring, cessation of breathing and frequent
arousals during sleep. They were aged between 6 to
12 years old.
The diagnosis of adenoid hypertrophy was based
on endoscopic nasopharyngeal findings (the occlusion
degree of the choana with adenoid tissue) and lateral
cephalometric X-ray findings (the thickness of soft
tissue density in nasopharyngeal airway) in patients
312 The European Research Journal
Volume 5
Issue 2
March 2019
Eur Res J 2019;5(2):311-318
Solmaz et al
suspected of having adenoid hypertrophy (i.e., having
nasal obstruction without septoconchal pathology,
snoring, and/or nasal discharge).
The inclusion criteria were as follows:
1. Patients aged between 6 to 12 years old,
2. With a diagnosis of adenoid hypertrophy
without tonsillar hypertrophy for a minimum of 12
months,
3. With a follow-up period of 2 months and per 2-
week intervals,
4. No sign of improvement despite medical
treatment with antibiotics under parental control.
The exclusion criteria were as follows:
1. Use of any nasal or systemic steroid within the
past 1 year.
2. Use of any nasal decongestant or anti-allergic
medication within the past 2 weeks.
3. History of upper respiratory tract infection
within the past 2 weeks.
4. History of one or more of the following
conditions: genetic craniofacial, or neuromuscular
syndromes, chronic epistaxis, immune disease,
asthma, nasal surgery, septal perforation, nasal trauma
within the last 3 months and hypersensitivity to
mometazon furoat.
The patients with a diagnosis of adenoid
hypertrophy who were candidates for surgery with a
6-weeks follow-up saline solution (3-5 drops, three
times/day) treatment were included in the study as
control group.
After taking a detailed medical history, the
symptoms were graded according to the severity of
patient’s clinic. Pre-treatment a lateral cephalometric
X-ray graph and a nasopharyngoscopic image (“MSI
Flexible Nasopharyngoscope, Germany” attached to
“Karl-Storz Telecam SL II, Tuttlingen, Germany”
camera) were obtained from every patient. The
hypertrophy of adenoid tissue was graded. Follow up
examinations were based on nasopharyngoscopic
records. Nasopharyngoscopic examination records
were repeated after medical treatment. The difference
between pretreatment and post treatment adenoid
tissue enlargement were compared.
Diagnostic Criteria
Symptoms
Nasal obstruction, snoring, and nasal discharge
The European Research Journal
Volume 5
Issue 2
March 2019 313
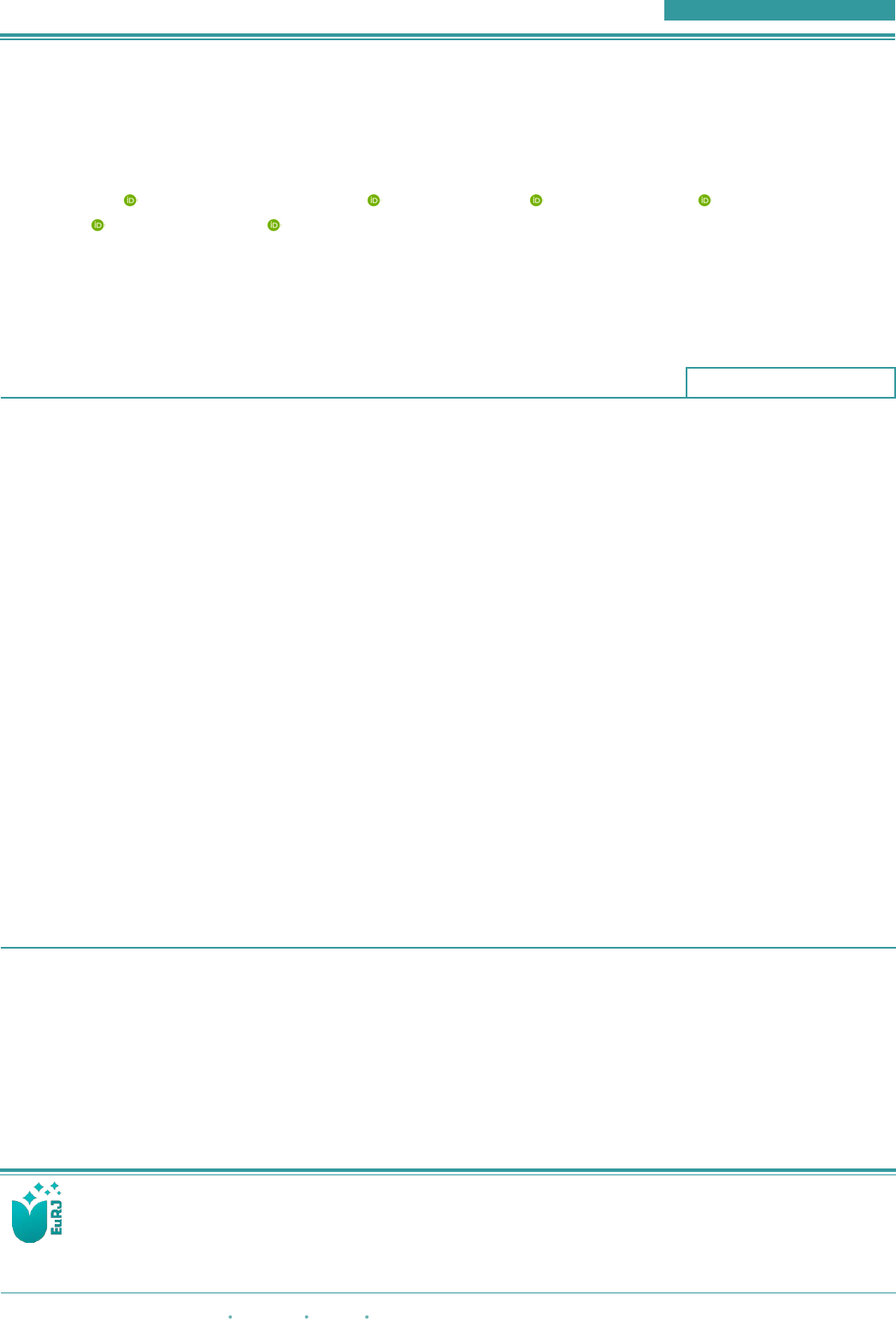
Figure A.Adeno/nasopharyngeal ratio according to the Fujioka method.
Eur Res J 2019;5(2):311-318 Topical nasal steroid and adenoid hypertrophy
were graded according to the frequency reported by
the parents (Grade 0: never seen, Grade 1: seen during
URTI, Grade 2: frequently seen, Grade 3: always
occurs).
Nasopharyngeal X-ray
Adenoid tissue enlargement was graded according
to the Adenoidal-nasopharyngeal ratios (ANR). The
distance of adenoid tissue density was measured along
a line dropped perpendicularly from point of maximal
convexity of adenoid tissue to its point of intersection
with line drawn along the straight part of the anterior
margin of the basiocciput. Then the nasopharyngeal
space was measured as the distance between posterior
superior edge of hard palate and the anterior inferior
edge of the spheno basioccipital synchondrosis. The
ANR was obtained by dividing the measurement for
adenoid tissue density by the value for nasopharyngeal
space in millimeters as described by Fujioka et al.
[19]. It was rated as: Grade 1: > 6 mm, Grade 2: 4-6
mm, and Grade 3: < 3 mm. Nasal endoscopy:
Performed with a Flexible Nasopharyngoscope
following topical anesthesia with 4% lidocaine
without any decongestant. Graded according to the
rate of obstruction of the choanal aperture by the
adenoid tissue as Grade 1: 25%, Grade 2: 50%, Grade
3: 75%, and Grade 4: 100% occlusion.
Adeno/nasopharyngeal ratio according to the Fujioka
method has been indicated in Figure A.
The children with a diagnosis of adenoidal
hypertrophy were then prescribed topical mometasone
furoate for 6 weeks, once a day, two puff to each
nostril (50 mcg/puff), comprising a daily total dose of
200 mcg. The nasal endoscopic evaluations were
repeated 6 weeks after the initial diagnostic workup.
Operation were not recommended to the control and
study groups with grade 2 adenoid hypertrophy,
however medical treatment was given.
Statistical Analysis
The data were analyzed with the SPSS for
Windows v.16.0 software by IBM, USA.using the
appropriate nonparametric tests for nominal and
ordinal data. In all analytical evaluations, p < 0.05 was
the significance limit value.
RESULTS
The study consisted of 75 patients (42 male, 33
female) with adenoid hypertrophy aged between 6 to
12 years old. Demographic characteristics and Body
Mass Index (BMI) and Percentiles of the study group
and the control group have been indicated in Table 1.
Fifty-five patients (30 male, 25 female) who had
topical nasal steroid accepted as study group and 20
patients (12 male, 8 female) who had preoperative
follow up record for 6-weeks were accepted as control
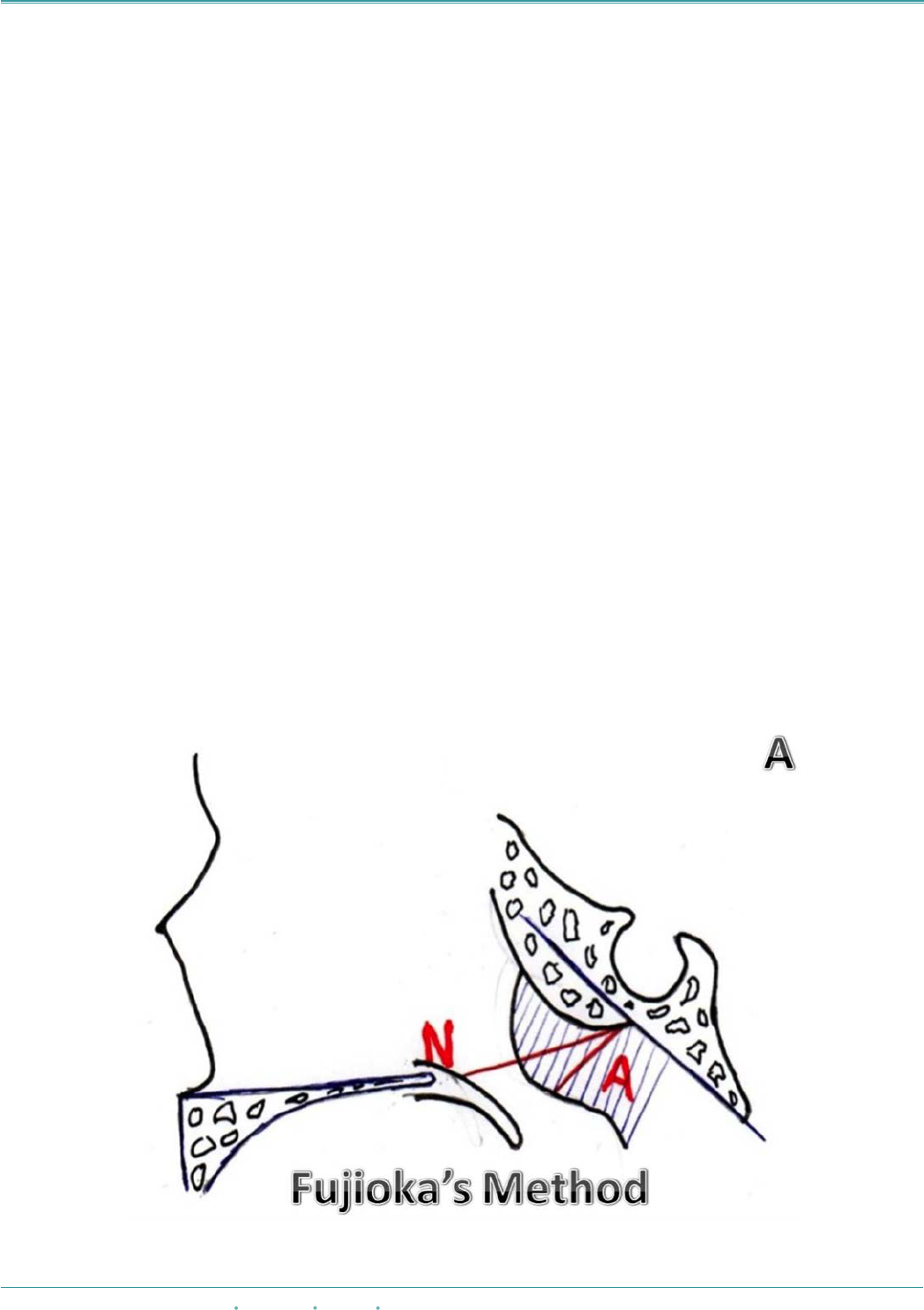
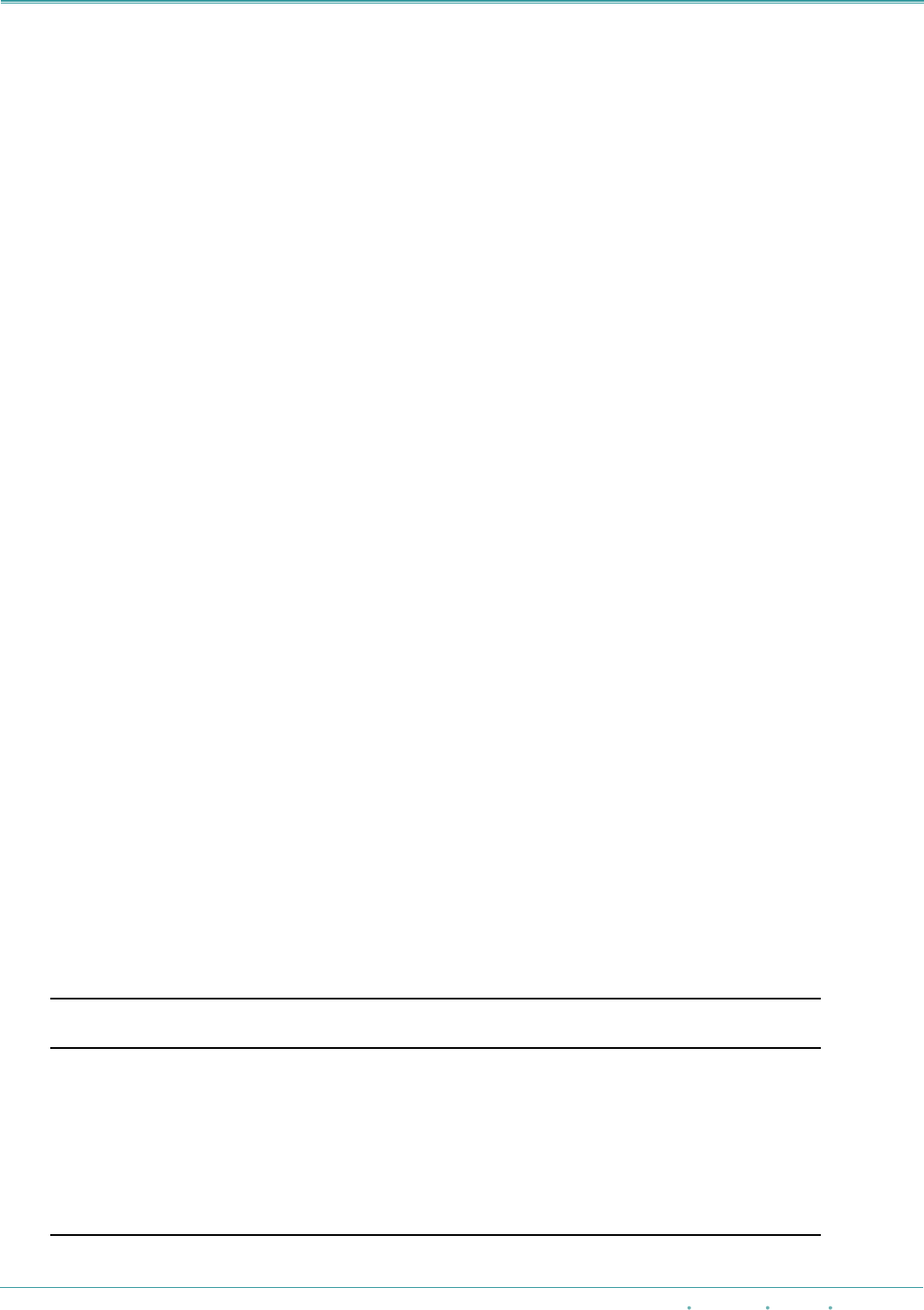
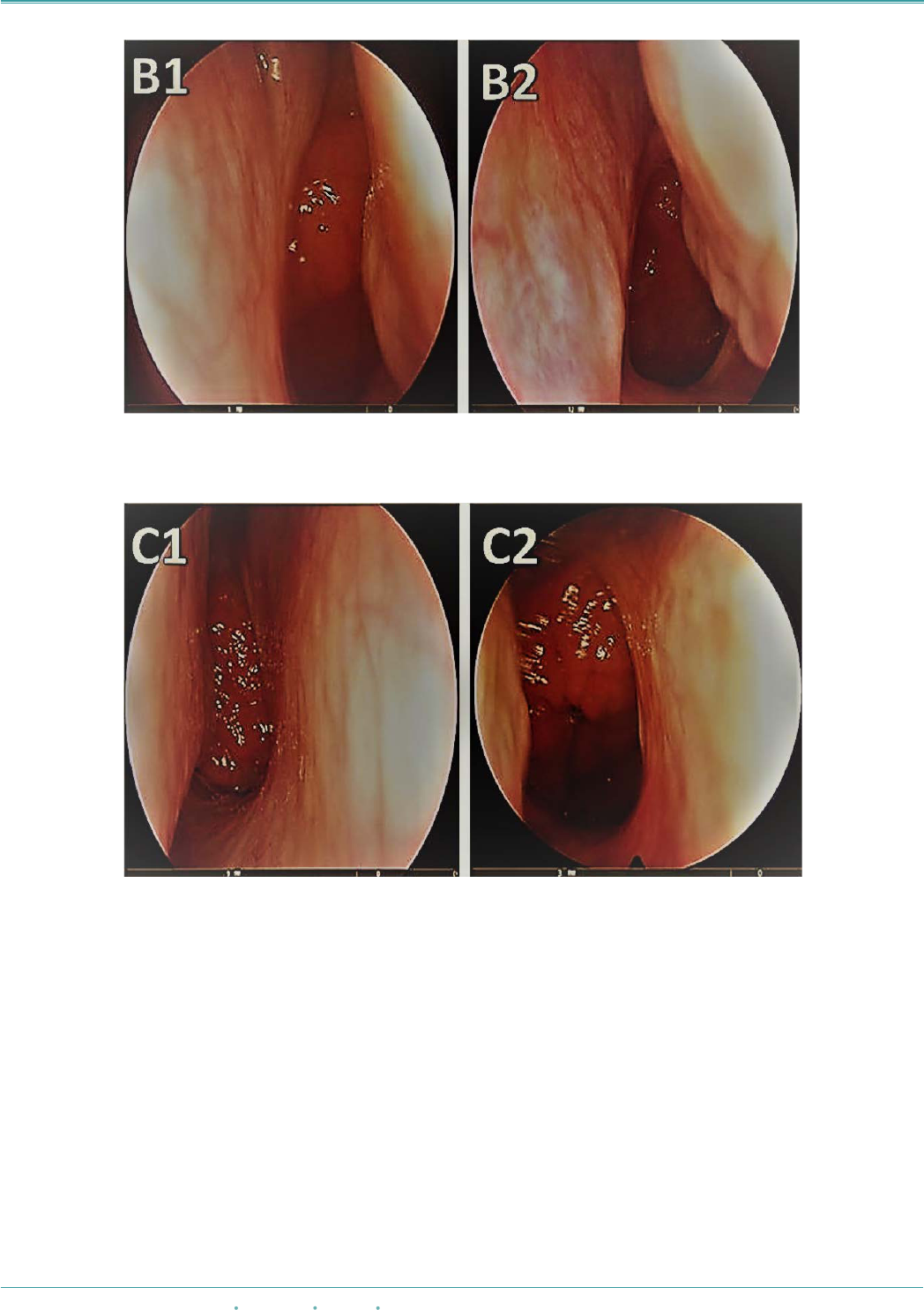
group. Endoscopic appearances before and after
topical steroid treatment were indicated in Figures B,
C and D.
The study group consisting of 30 males and 25
females was administered topical nasal Mometasone
Furoate steroid treatment. Nasopharyngeal X-rays
before treatment revealed that 25 patients were Grade
2 and 30 patients were Grade 3 grade according to the
Fujioka method. Flexible endoscopy performed before
the treatment revealed that 20 patients were Grade 2,
11 patients were Grade 3 and 24 patients were Grade
4. Nasal endoscopies performed after 6 weeks of
314 The European Research Journal
Volume 5
Issue 2
March 2019
Table 1. Demographic characteristics and BMI and percentiles of the study group and the control group
Study Group
(n = 55)
Control Group
(n = 20)
Age (year)
7.92 ± 1.81
(6-12)
7.80 ± 1.36
(6-11)
Gender (M/F)
30/25
12/08
Height (cm)
125.47 ± 11.30
123.15 ± 6.89
Weight (kg)
28.72 ± 7.09
27.55 ± 5.88
BMI
17.94 ± 1.58
17.95 ± 1.94
Percentile
77.89 ± 16.88
78.95 ± 13.83
BMI as a multiple of the mean
BMI
1.11 ± 0.07
1.10 ± 0.08
BMI = Body Mass Index, F = Female, M = Male
!
Eur Res J 2019;5(2):311-318
Solmaz et al
intranasal topical steroid therapy revealed that 45
patients were Grade 1 and 10 patients were Grade 2.
Nasopharyngeal X-rays were not requested for follow-
up to avoid the additional harmful effects of X-rays.
A statistically significant difference was present
between endoscopic grades before and after treatment
(p < 0.0001) (Table 2). Non-severe epistaxis was
observed in three patients who administrated topical
steroid therapy.
The 20 patients in the control group where saline
solution (0.9 % NaCl) treatment was administered
consisted of 12 males and 8 females. Nine patients was
Grade 2 and Grade 3 in 11 patients on nasopharyngeal
X-rays at first presentation according to the Fujioka
method in this group. Flexible nasal endoscopy
performed simultaneously revealed that there were
Grade 2 in 6 patients, Grade 3 in 9 patients and Grade
4 in 5 patients. Nasal endoscopies performed after 6
weeks in control group receiving saline solution
treatment revealed Grade 2 in 7 patients, Grade 3 in
10 patients and Grade 4 in 3 patients. There was no
statistically significant difference between in the prior
and later grades of the control group (p = 0.3125)
(Table 2).
The European Research Journal
Volume 5
Issue 2
March 2019 315
Figure B. Endoscopic appearance before (B1) and after (B2) topical steroid treatment.
Figure C. Endoscopic appearance before (C1) and after (C2) topical steroid treatment.
Eur Res J 2019;5(2):311-318 Topical nasal steroid and adenoid hypertrophy
DISCUSSION
Demain and Goetz [20] used beclomethasone
nasal spray for 8 weeks (338 microgm/day) followed
by a lower daily dose (168 microgm/day) in the next
16 weeks for the treatment of adenoid hypertrophy and
reported a decrease in adenoid size in all the study
subjects. A history of atopy was reported in previous
studies but they excluded those with such a history in
this study [20]. We treated 55 children between the
ages of 6 and 12 years with mometasone furoate nasal
spray at a daily dose of 200 mcg for 4 weeks [20].
Lepcha et al. [21] reported no significant improvement
in X-ray and endoscopy findings of subjects
administered intranasal topical beclomethasone for 8
weeks while there was a 6% improvement in nasal
congestion. However, there was an improvement in
adenoidal obstruction and clinical findings when
compared with placebo after 24 weeks of treatment
[21]. In our patients, we also observed a decrease in
the endoscopic findings of adenoid tissues.
Kheirandish-Gozal and Gozal [4] showed
intranasal budesonide to decrease the severity of
respiratory distress and the size of the adenoids,
although mildly, with 6 weeks of use in children with
mild OSA. Brouillette et al. [17] observed an
improvement in the respiration of patients despite no
noticeable change in the adenoid tissue mass after 6
weeks of treatment with intranasal fluticasone before
T&A surgery in patients with moderate-to-heavy
OSA. No significant change was found in the size of
adenoids and tonsils and in the symptoms as reported
by the parents but there was a significant reduction in
apnea and hypopnea frequency among children treated
with fluticasone.
Similar positive effects in OSA patients were
reported in later studies. It is interesting that the effect
on OSA symptoms continued even after the treatment
was discontinued during 9 months of follow-up in the
Alexopoulos et al. [18] study on 27 patients. The
general results regarding OSA severity are strikingly
similar despite differences in patient selection criteria
316 The European Research Journal
Volume 5
Issue 2
March 2019
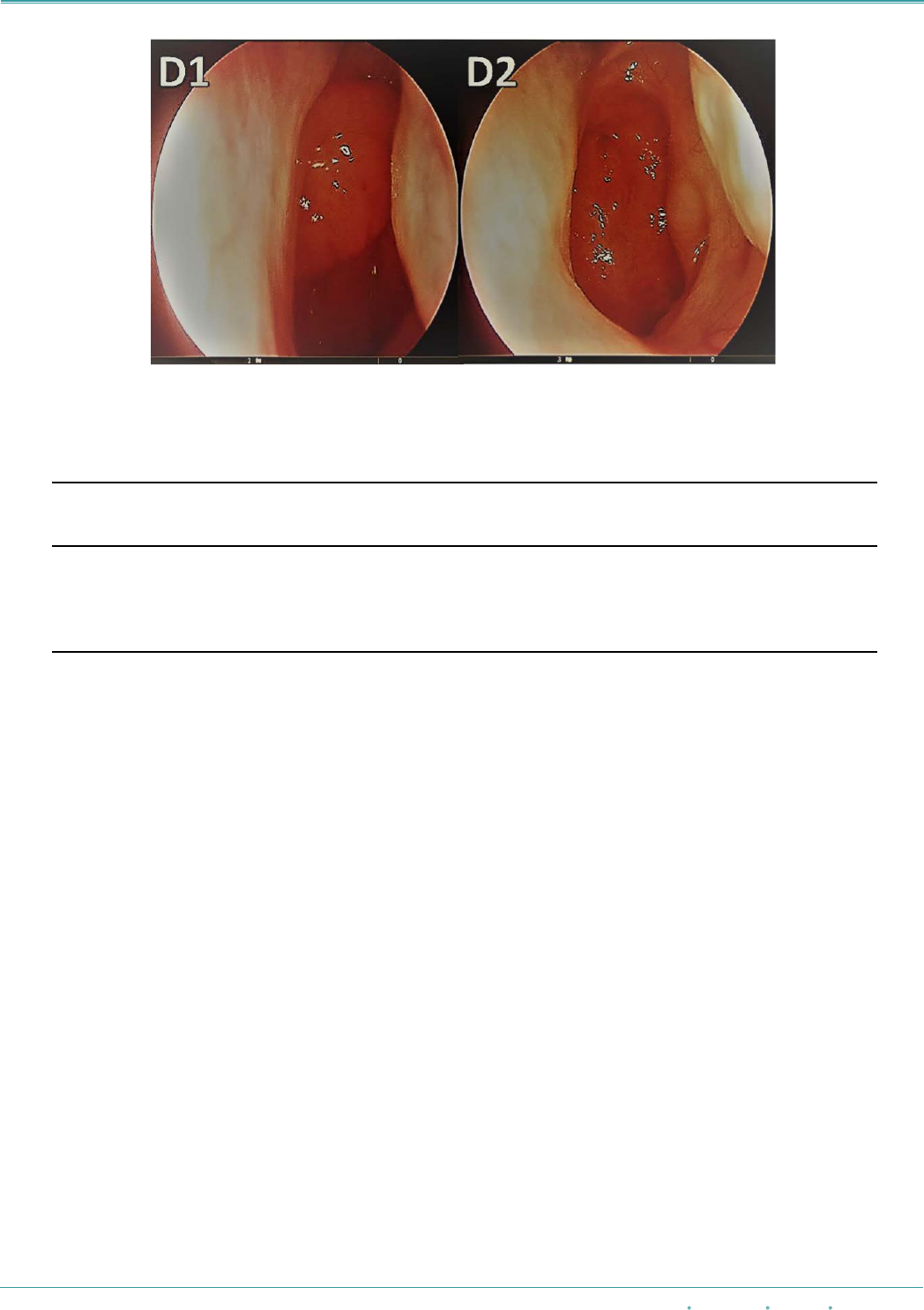
Figure D. Endoscopic appearance before (D1) and after (D2) topical steroid treatment.
Table 2. First and second endoscopic grades in the study group and in the control group
Grade
n (%)
Study
(n = 55)
First
Study
(n = 55)
Second
Control
(n = 20)
First
Control
(n = 20)
Second
Grade 1
0 (0%)
45 (81%)
0 (0%)
0 (0%)
Grade 2
20 (36%)
10 (18%)
6 (30%)
7 (35%)
Grade 3
11 (20%)
0 (0%)
9 (45%)
10 (50%)
Grade 4
24 (43%)
0 (0%)
5 (25%)
3 (15%)
Endoscopic grade (mean ± SD)
3.07 ± 0.89
1.18 ± 0.38
2.95 ± 0.75
2.80 ± 0.69
*Wilcoxon test (paired samples).
!

Eur Res J 2019;5(2):311-318
Solmaz et al
and treatment methods, indicating that nasal
corticosteroids can be used as the first treatment option
in pediatric OSA. However, there is no clear
consensus on the appropriate steroid dosage and
treatment duration at present [16, 22]. Junk et al. [23]
have reported a significant improvement in loud
snoring, breath holding, frequent awakening from
sleep, breathing from the mouth, URTI frequency and
nasal discharge after 4 weeks of intranasal
mometasone furoate treatment in children. We also
chose mometasone furoate among the various steroid
nasal sprays commercially available for this study. The
reason was the absence of reports on any negative
effect of this spray on the nasal mucosa or side effects
related to the hypothalamus-pituitary-adrenal axis and
growth with long-term use [24]. The systemic effect
of the drug is lower than other steroids after topical
administration [25]. Berlucchi et al. [26] recently
evaluated the effectiveness of 40 days of mometasone
furoate treatment in adenoid hypertrophy and found
symptomatic improvement in 77.7% of the patients.
Fujioka et al. [19] described the A/N ratio as an
indicator of adenoid hypertrophy in 1979 and the
method has been used in many studies. Jung et al. [23]
showed that the A/N ratio on lateral neck graphs
decreased in 22 (71%) of 31 children after 4 weeks of
treatment (p = 0.006). Cengel and Akyol [27] reported
shrinkage of adenoid tissue in 67.2% of the children
after 6 weeks of treatment with intranasal mometasone
furoate treatment in 2006. However, there is no proven
mechanism explaining adenoid shrinkage. The
presence of inflammation in the soft palate mucosal
surface has been shown in OSA patients [28]. Jung et
al. [23] thought that this type of upper respiratory tract
inflammation could also involve the adenoid mucosa
and that 4 weeks of local steroids could decrease this
inflammation, causing the adenoids to shrink.
There are several methods to evaluate the size of
the adenoids causing sleep-disordered breathing. The
most commonly used techniques are lateral neck
radiograph and direct videorhinoscopy. Mlynarek et
al. [29] reported video rhinoscopy to be more useful
for the evaluation of symptom severity in 2004.
However, the nasopharyngeal examination of small
children with fiberoptic devices can be difficult. The
above results indicate that intranasal steroids can be
used to reduce symptoms in children with sleep-
disordered breathing, regardless of allergy or sinusitis.
The results of our study were also consistent with the
literature. However, a limitation of our study is the
lack nasal airway patency evaluation with objective
methods such as acoustic rhinometry.
CONCLUSION
We believe that the use of intranasal steroids
(mometasone furoate) for 6 weeks in patients with
pediatric chronic nasal obstruction due to adenoid
hypertrophy may be an effective treatment modality
in alleviating symptoms and decreasing adenoid
volume without causing systemic side effects.
Placebo-controlled studies are required to investigate
the long-term effect of short-term steroid use in the
treatment of pediatric sleep disorders in the future.
Conflict of interest
The authors disclosed no conflict of interest during
the preparation or publication of this manuscript.
Financing
The authors disclosed that they did not receive any
grant during conduction or writing of this study.
REFERENCES
[1] Lumeng JC, Chervin RD. Epidemiology of pediatric
obstructive sleep apnea. Proc Am Thorac Soc 2008;5:242-52.
[2] O’Brien LM, Holbrook CR, Mervis CB. Sleep and
neurobehavioral characteristics of 5- to 7-year-old children with
parentally reported symptoms of attention-deficit/hyperactivity
disorder. Pediatrics 2003;111:554-63.
[3] Blunden S, Lushington K, Lorenzen B, Wong J, Balendran
R, Kennedy D. Symptoms of sleep breathing disorders in children
are underreported by parents at general practice visits. Sleep
Breath 2003;7:167-76.
[4] Kheirandish-Gozal L, Gozal D. Intranasal budesonide
treatment for children with mild obstructive sleep apnea
syndrome. Pediatrics 2008;122;e149-55.
[5] Marcus CL. Sleep-disordered breathing in children. Am J
Respir Crit Care Med 2001;164:16-30.
[6] Raphael G, Kaliner M. The tonsils and adenoids: Allergy and
the pharyngeal lymphoid tissue. In Otolaryngologic Clinics of
North America. Edited by Kornblut AD, Saunders WB:
Philadelphia, 1987:pp. 295-303.
[7] Capdevila OS, Kheirandish-Gozal L, Dayyat E, Gozal D.
Pediatric obstructive sleep apnea: complications, management,
and long-term outcomes. Proc Am Thorac Soc 2008;5:274-82.
The European Research Journal
Volume 5
Issue 2
March 2019 317

Eur Res J 2019;5(2):311-318 Topical nasal steroid and adenoid hypertrophy
[8] Cowan DL, Hibbert J. Tonsils and adenoids: In Scott Browns
Pediatric Otolaryngology (Vol. 6) 6th edition. Edited by Kerr AG,
Adams DA, Cinnamond MJ. Butterworth Heinemann, Oxford
Chpt 1997;18, p.4-8.
[9] Li AM, Wong E, Kew J, Hui S, Fok TF. Use of tonsil size in
the evaluation of obstructive sleep apnoea. Arch Dis Child
2002;87:156-9.
[10] Schechter MS. Technical report: diagnosis and management
of childhood obstructive sleep apnea syndrome. Section on
Pediatric Pulmonology, Subcommittee on Obstructive Sleep
Apnea Syndrome. Pediatrics 2002;109: e69.
[11] American Academy of Pediatrics. Clinical practice
guideline: diagnosis and management of childhood obstructive
sleep apnea syndrome. Pediatrics 2002;109:704-12.
[12] Brodsky L. Modern assessment of tonsil and adenoids.
Pediatr Clin North Am 1989;36:1551-69.
[13] Tracy JM, Demain JG, Hoffman KM, Goetz DW. Intranasal
beclomethasone as an adjuvant to treatment of chronic middle
ear effusion. Ann Allergy Asthma Immunol 1998;80:198-206.
[14] Brannan MD, Herron JM, Affrime MB. Safety and
tolerability of once-daily mometasone furoate aqueous nasal
spray in children. Clin Ther 1997;19:1330-9.
[15] Kheirandish-Gozal L, Serpero LD, Dayyat E, Kim J,
Goldman JL, Snow A. Corticosteroids suppress in vitro tonsillar
proliferation in children with obstructive sleep apnoea. Eur
Respir J 2009;33:1077-84.
[16] Goldbart AD, Goldman JL, Veling MC, Gozal D.
Leukotriene modifier therapy for mild sleep disordered breathing
in children. Am J Respir Crit Care Med 2005;172:364-70.
[17] Brouillette RT, Manoukian JJ, Ducharme FM, Oudjhane K,
Earle LG, Ladan S. Efficacy of fluticasone nasal spray for
pediatric obstructive sleep apnea. J Pediatr 2001;138:838-44.
[18] Alexopoulos EI, Kaditis AG, Kalampouka E, Kostadima E,
Angelopoulos NV, Mikraki V. Nasal corticosteroids for children
with snoring. Pediatr Pulmonol 2004;38:161-7.
[19] Fujioka M, Young LW, Girdany BR. Radiographic
evaluation of adenoidal size in children: adenoidal-
nasopharyngeal ratio. Am J Roentgenol 1979;133:401-4.
[20] Demain JG, Goetz DW. Pediatric adenoidal hypertrophy and
nasal airway obstruction: reduction with aqueous nasal
beclomethasone. Pediatrics 1995;95:355-64.
[21] Lepcha A, Kurien M, Job A, Jeyaseelan L, Kurien T. Chronic
adenoid hypertrophy in children - is steroid nasal spray
beneficial? Indian J Otolaryngol Head Neck Surg 2002;54:280-
4.
[22] Kheirandish L, Goldbart AD, Gozal D. Intranasal steroids
and oral leukotriene modifier therapy in residual sleep-disordered
breathing following tonsillectomy and adenoidectomy in
children. Pediatrics 2006;117:e61-6.
[23] Jung YG, Kim HY, Min JY, Hun JD, Seung KC. Role of
intranasal topical steroid in pediatric sleep disordered breathing
and influence of allergy, sinusitis, and obesity on treatment
outcome. Clin and Exp Otorhinolaryngol 2011;4:27-32.
[24] Minshall E, Ghaffar O, Cameron L, O’Brien F, Quinn H,
Rowe-Jones J. Assessment by nasal biopsy of long-term use of
mometasone furoate aqueous nasal spray (Nasonex) in the
treatment of perennial rhinitis. Otolaryngol Head Neck Surg
1998;118:648-54.
[25] Boner AL. Effects of intranasal corticosteroids on the
hypothalamic-pituitary-adrenal axis in children. J Allergy Clin
Immunol 2001;108:32-9.
[26] Berlucchi M, Salsi D, Valetti L, Parrinello G, Nicolai P. The
role of mometasone furoate aqueous nasal spray in the treatment
of adenoidal hypertrophy in the pediatric age group: preliminary
results of a prospective, randomized study. Pediatrics
2007;119:e1392-7.
[27] Cengel S, Akyol MU. The role of topical nasal steroids in
the treament of children with otitis media with effusion and/or
adenoid hypertrophy. Int J Pediatr Otorhinolaryngol
2006;70:639-45.
[28] Kimoff RJ, Hamid Q, Divangahi M, Hussain S, Bao W, Naor
N. Increased upper airway cytokines and oxidative stress in
severe obstructive sleep apnoea. Eur Respir J 2011;38:89-97.
[29] Mlynarek A, Tewfik MA, Hagr A, Manoukian JJ, Schloss
MD, Tewfik TL. Lateral neck radiography versus direct video
rhinoscopy in assessing adenoid size. J Otolaryngol 2004;33:360-
5.
318 The European Research Journal
Volume 5
Issue 2
March 2019
This is an open access article distributed under the terms of Creative Common
Attribution-NonCommercial-NoDerivatives 4.0 International License.
